
In Trenton, the debate over nurse practitioner independence is being framed as a question of patient safety. But beneath the floor statements and executive orders lies something more consequential:
Institutional power.
When Executive Order No. 415 terminated the State of Emergency first declared under Executive Order No. 103, it set in motion the reinstatement of physician collaboration requirements that had been suspended for nearly six years. Only days before that reinstatement, Mikie Sherrill issued Executive Order No. 13, granting a 45-day reprieve while lawmakers consider Senate Bill No. 2996.
The public narrative is about continuity of care.
The private tension is about control.
The Physician Voice at the Table
At the center of the controversy is Dr. Tanisha Arora, now serving as President of the New Jersey Chapter of the American College of Emergency Physicians (NJACEP).
NJACEP represents emergency physicians. Its mission is advocacy for physician interests in emergency care policy.
S2996 proposes eliminating mandatory joint protocols for experienced Advanced Practice Nurses (APNs). Those protocols legally tether nurse practitioners to collaborating physicians — relationships that can carry financial and professional leverage.
When the head of a physician advocacy organization influences amendments to legislation that would loosen physician control over nurse practitioners, the issue is not legality.
It is structural conflict of interest.
Even if her input is grounded in legitimate clinical concerns, the institutional alignment is unmistakable.
“Nurses Should Be More Educated”
In discussions surrounding amendments to S2996, physician advocates have emphasized educational disparities between medical doctors and nurse practitioners. Dr. Arora has been publicly associated with the position that expanded autonomy should be tied to higher educational thresholds — summarized by some observers as the assertion that nurses “should be more educated” before practicing independently.
While the precise wording must be confirmed through official transcripts or written submissions, the framing itself is not uncommon in physician-led policy arguments:
Autonomy must be conditioned on additional education.
On its surface, that position sounds reasonable. Education is foundational to safe care.
But when inserted into legislation, it becomes a gatekeeping mechanism.
If new educational benchmarks are layered into statute:
- Independence can be delayed.
- Existing practitioners may be excluded.
- Market access becomes contingent on credentialing structures influenced by physician boards.
The debate shifts from performance during six years of independent operation to credential escalation.
And that shift matters.
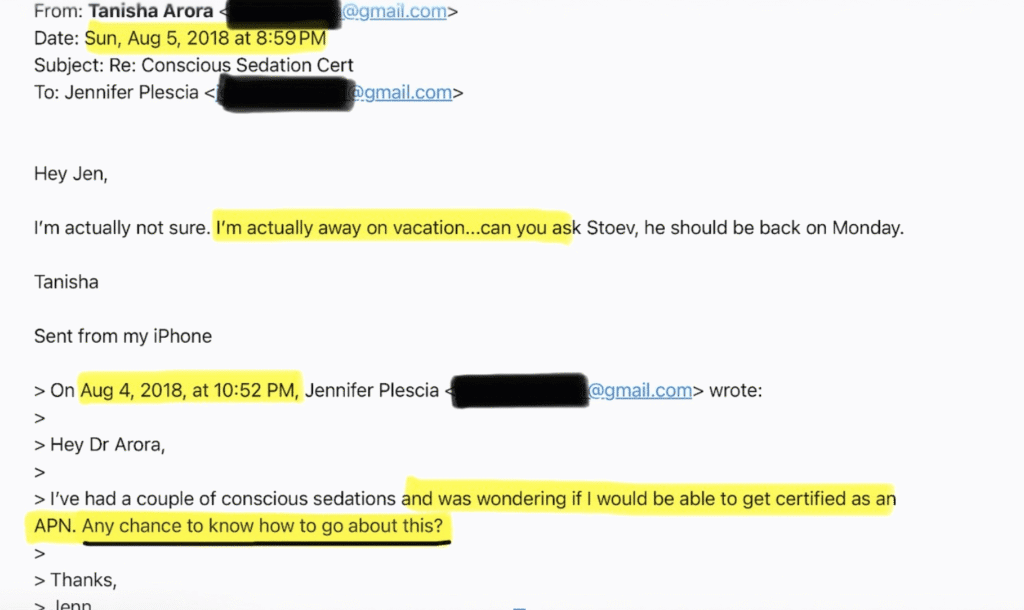
Image credit: Bridget Mulroy
A Thread That Predates the Legislation
Years before this legislative battle, Jenn Plescia — founder of IVs By The Seas — reached out to Dr. Arora (via email — pictured) about the process and education of becoming a nurse practitioner. At the time Plescia reached out, she was still a nurse working in the ER. Dr. Arora was the ER doctor she reached out to about furthering her education. In that email, Plescia sought guidance from Dr. Arora about acquiring her certification as a NP and advancing her career.
At the time, it was a routine professional inquiry.
Today, viewed against the backdrop of S2996 and EO 13, the chronology takes on new dimension:
A nurse entrepreneur once seeking mentorship from a physician leader now finds her business model directly affected by legislation shaped, in part, by physician advocacy leadership.
There is no allegation of impropriety in that contact.
But the optics are unavoidable.
When a former point of professional inquiry later becomes a stakeholder in legislation influenced by the same physician leader — now elevated to head of a statewide advocacy body — questions arise about proximity, power, and perspective.
The Legislative Flaw
The deeper issue is not personal. It is procedural.
New Jersey’s legislative process permits professional advocacy groups to shape amendments without structural safeguards against institutional self-interest.
Physician organizations may testify on nurse scope expansion.
Nurse organizations may counter.
Economic implications remain embedded beneath clinical rhetoric.
But nowhere in that process is there a neutral balancing mechanism requiring disclosure of economic impact on competing professional groups.
Joint protocols are not merely safety tools.
They are business relationships.
When legislation determining their elimination is influenced by leaders of organizations whose members financially benefit from their continuation, the absence of formal conflict-of-interest guardrails becomes a systemic flaw.
The public hears “education standards.”
The marketplace hears “control.”
What Is Really Being Decided
For nearly six years, thousands of APNs practiced without mandatory joint protocols. Clinics opened. Patients were treated. Emergency rooms were relieved of volume.
If independence was unsafe, the data should show it.
Instead, the debate has pivoted toward credential recalibration.
S2996’s proposed experience threshold — 24 months or 2,400 hours — reflects a compromise model. But if amendments influenced by physician leadership layer additional educational barriers, the reform risks becoming symbolic rather than substantive.
Executive Order 13 bought 45 days.
It did not resolve the institutional tug-of-war.
Beyond Personalities
This is not an accusation.
It is an examination of structure.
When advocacy leaders with clear professional stakes influence legislation governing economic competitors, transparency and balance are essential.
Without them, policy begins to look less like patient-centered reform and more like negotiated preservation of hierarchy.
As April 2 approaches, New Jersey is not merely deciding whether nurse practitioners can practice independently.
It is deciding whether healthcare regulation will reflect demonstrated performance — or entrenched institutional power.
And in that decision, influence matters.
Links:
Executive Order 102:
https://www.nj.gov/infobank/eo/056murphy/pdf/EO-102.pdf
Executive Order 112:
https://www.nj.gov/infobank/eo/056murphy/pdf/EO-112.pdf
Executive Order 292:
https://nj.gov/infobank/eo/056murphy/pdf/EO-292.pdf
Executive Order 415:
https://nj.gov/infobank/eo/056murphy/pdf/EO-415.pdf
IVs By The Seas Statement:
https://www.ivsbytheseas.com/help
Senate Bill S2996:
https://www.njleg.state.nj.us/bill-search/2026/S2996
IVs By The Seas Instagram
https://www.instagram.com/ivsbytheseas/
IVs By The Seas Website




{kind=link}